Pediatric Acute Myeloid Leukemia
Disease information
Treatment
Previously, the mainstay of treatment for pediatric acute myeloid leukemia (AML) was allogeneic hematopoietic stem cell transplantation. Now, treatment approaches are increasingly personalized, with strategies being adjusted according to prognostic categories and individual responses to therapy. This shift allows for more targeted and potentially more effective treatments for children with AML.
The standard induction therapy for acute myeloid leukemia (AML) typically includes the '7+3' regimen, which involves seven days of continuous infusion of cytarabine (Ara-C) and three days of idarubicin. Similarly to acute lymphoblastic leukemia (ALL), it is also crucial to prevent a relapse in the central nervous system by administering intrathecal chemotherapy.
The effectiveness of chemotherapy is judged by achieving complete remission. This is defined as having less than 5% blasts in the bone marrow, no detectable leukemia cells in the peripheral blood, and normal recovery of blood cell counts (a neutrophil count above 1,500/mm3 and a platelet count above 100,000/mm3). Additionally, any extramedullary disease, which refers to leukemia involvement outside of the bone marrow, should be resolved. It's important to understand that complete remission is not the same as a cure. Once complete remission is reached, post-remission therapy is initiated to maintain the remission state. If complete remission is not achieved, then re-induction therapy may be necessary.
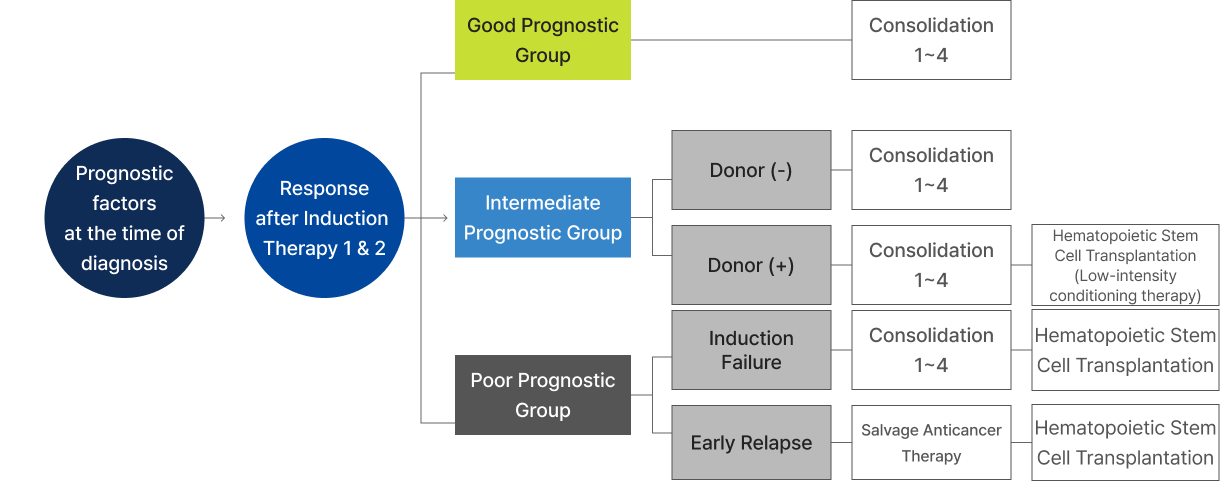
Following initial treatment that induces complete remission, a substantial number of leukemia cells, estimated to be between 100 million and 1 billion, may still remain undetectable by microscopy. To prevent a relapse and move toward a cure, post-remission treatment is carefully planned based on a thorough assessment of the patient's prognosis, their risk category, and the availability of a suitable donor for transplantation if necessary. This tailored approach is key to optimizing long-term outcomes for patients with leukemia.
-
①
Consolidation Chemotherapy
- For the group with a good prognosis, a total of six chemotherapy treatments, including induction therapy, are performed with drugs containing cytarabine, idarubicin, etoposide, and mitoxantrone.
-
②
Hematopoietic Stem Cell Transplantation
- Except for cases with a good prognosis that continue with just some chemotherapy, once remission occurs, consolidation therapy is performed while conducting HLA testing to find a donor. If an appropriate donor is found, hematopoietic stem cell transplantation is performed. This is performed in the state of first remission after a total of 3-6 rounds of chemotherapy, including consolidation therapy.
If a patient requiring hematopoietic stem cell transplantation has a sibling with a matching HLA profile, this sibling is typically the preferred donor. If a sibling match is not available, if the HLA match is not suitable, or if the sibling is unable to donate for other reasons, a search for an unrelated donor is conducted through Korea's National Organ Transplant Management Center (KONOS). Should a compatible HLA donor not be located, alternative options like cord blood transplantation, which uses stem cells from umbilical cord blood, or haploidentical transplantation, where the donor is a half-match often a family member, may be considered. The decision to proceed with hematopoietic stem cell transplantation takes into account the potential side effects and risks associated with the procedure. This decision is made after careful evaluation of the benefits and potential drawbacks in relation to the patient's particular condition and the availability of a suitable donor.
Acute promyelocytic leukemia (APL) cells release substances that can trigger coagulation within the blood vessels, leading to conditions such as disseminated intravascular coagulation (DIC), which includes a reduction in fibrinogen levels. This can result in significant bleeding events, such as gastrointestinal, respiratory, or even brain hemorrhages. It's crucial to begin treatment with All-trans-retinoic acid (ATRA) orally as quickly as possible if APL is suspected, even before genetic confirmation, to promote the maturation of the leukemia cells into normal blood cells and to prevent early death from bleeding through aggressive transfusion support.
In the diagnosis of APL, a specific genetic test is done to look for a translocation between the PML gene on chromosome 15 and the RARα gene on chromosome 17, resulting in the PML/RARα fusion gene, t(15;17), which is present in the majority of APL cases. For induction therapy, ATRA is used in combination with anthracycline-based chemotherapy. This is followed by three cycles of consolidation chemotherapy and then two years of maintenance therapy with oral anticancer agents and periodic ATRA administration.