Immune thrombocytopenic purpura (ITP)
Disease information
Overview
Thrombocytopenia happens when there's a drop in the number of platelets in your blood. These are the tiny cells that help stop bleeding by making your blood clot. Normally, you should have between 150,000 to 450,000 platelets per cubic millimeter of blood. When the count falls below 150,000, doctors start to watch out for signs of thrombocytopenia. If it goes below 100,000, it's often seen as a more serious case.
Doctors have ways to figure out why someone's platelet count is low, but sometimes, the exact cause is hard to pin down. In the past, when no cause could be found, it was called Idiopathic Thrombocytopenic Purpura (ITP). Nowadays, because we know the body's own defense system is often involved by mistakenly attacking platelets, it's more commonly called Immune Thrombocytopenic Purpura (ITP).
ITP is what doctors call it when they can't find a specific reason for the low platelets, like another illness or a reaction to medicine. Usually, the other blood cells, like white and red blood cells, are in the normal range. If thrombocytopenia goes away within six months, it's called acute; if it lasts longer, it's called chronic. In adults, ITP usually sticks around and doesn't go away on its own.
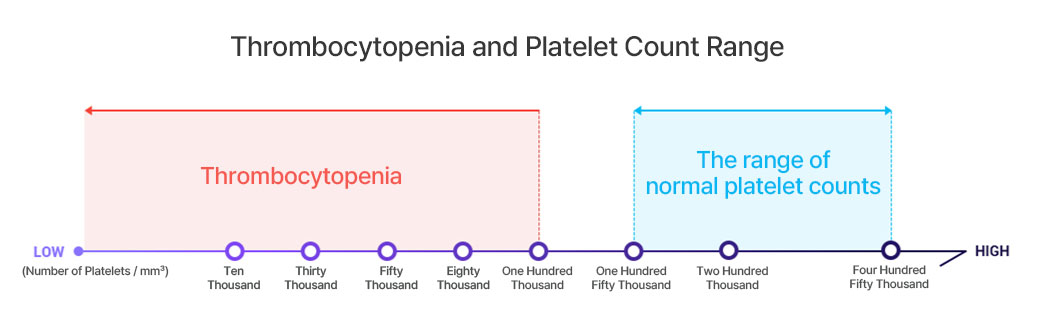
▲ Thrombocytopenia and Platelet Count Range
Causes & Symptoms
In Immune Thrombocytopenic Purpura (ITP), platelet counts are below normal, which can be due to two main reasons.
In Immune Thrombocytopenic Purpura (ITP), a key issue is that platelets – the cells that help blood clot – are destroyed faster than they should be. This happens because the body mistakenly makes antibodies that attack platelets. These antibodies stick to proteins on the platelets' surface. Once that happens, the platelets become targets for a type of white blood cell in the spleen, known as macrophages, which eat them up. Why the body starts making these platelet-attacking antibodies in the first place is still something of a mystery.
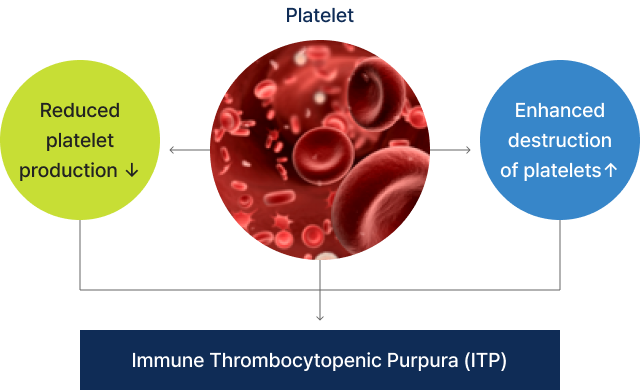
▲ Immune Thrombocytopenic Purpura (ITP)
Platelets are crucial blood cells made in the bone marrow that help keep bleeding in check—a process known as hemostasis. When you get a cut or a wound, platelets rush to the scene to form a clot and stop the bleeding. If your platelet count is low, it can make bleeding worse and disrupt the clotting process, leading to symptoms like more frequent or severe bruising, longer-lasting bleeding from cuts, spontaneous bleeding from the gums or nose, and in women, heavier menstrual flows.
- The appearance of petechiae or bruise-like hemorrhages on the skin
- Bleeding of the gums and oral mucosa
- Increased menstrual flow and prolonged duration of periods
- Epistaxis (nosebleed)
- Hematuria urine resembling the color of black tea
- In severe cases, the occurrence of cerebral hemorrhage
- Melena (blood in stool)
Many people with thrombocytopenia, a condition where platelet levels are lower than normal, don't show any signs of it, especially if their platelet count stays above 50,000 per cubic millimeter. They go about their daily lives without noticing any changes. However, bleeding issues are more likely to happen if the platelet count gets really low. There isn't a specific number that will tell doctors for sure if someone will have symptoms, but it's more likely to happen when the count drops below 20,000 to 30,000 per cubic millimeter.