Pediatric Lymphoma
Disease information
Overview
Lymphoma is a form of blood cancer that affects the lymphatic system, a crucial component of our immune defense. This system encompasses the network of lymph nodes, lymphatic vessels, lymphocytes (a type of white blood cell), as well as organs like the spleen, tonsils, thymus, and bone marrow.
Structurally akin to the circulatory system—which is made up of the heart, arteries, capillaries, and veins—the lymphatic system comprises lymph vessels and nodes through which lymph fluid circulates, carrying lymphocytes that help fight infection.
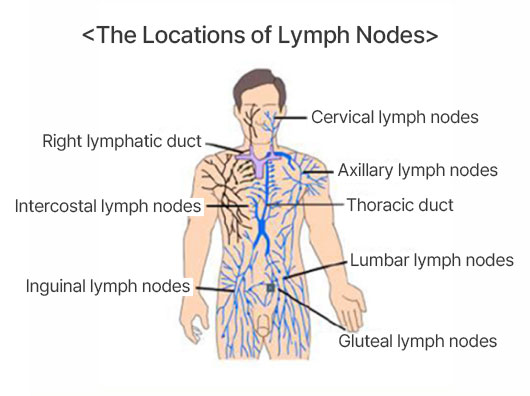
▲ Source: The Korean Society of Hematology
Lymph fluid is rich in white blood cells known as lymphocytes, and along the network of lymph vessels, there are small, bean-shaped clusters known as lymph nodes. Unique among blood cancers, lymphoma can form solid masses or tumors, similar to other solid cancers. In the pediatric population, lymphoma constitutes about 15% of all cancers, making it the third most common type of cancer in children, after leukemia and brain tumors. While lymphoma occurs in roughly 10% of childhood cancer cases, its prevalence increases significantly in adolescence, accounting for about one-third of all cancers in the 10 to 20-year-old age group.